Medication-related osteonecrosis of the jaw is a fairly serious drug reaction, resulting in the gradual death of jaw bone. Following oral and maxillofacial or periodontal surgery, or endodontic therapy it can result in significant complication due to the reduced healing ability of the bone.
MRONJ is caused by either antiresorptive drugs (including bisphosphonates) that cause a reduced ability for the reabsorption of bone, or antiangiogenic drugs, which impair the formation of new blood vessels. While uncommon, MRONJ is a serious side effect of these drugs, and extra awareness should be used when treating patients with these conditions.
There is no known effective prevention technique for MRONJ, therefore diligence in in watching for signs of MRONJ when treating patients on intravenous antiresorptive and/or antiangiogenic drugs is vital. Patients on these drugs for 3 years have an increased likelihood of developing MRONJ, and therefore increased awareness and caution should be exercised while treating them.
The following table from the AAOMS 2014 guidelines summarizes the clinical findings and treatment strategies for MRONJ:
| MRONJ Staging | Criteria* (>8 weeks) | Treatment Strategies** | Picture |
|---|---|---|---|
| At risk | No apparent necrotic bone in patients who have been treated with either oral or IV bisphosphonates | No treatment indicated, Patient education | N/A |
| Stage 0 | No clinical evidence of necrotic bone, but non-specific clinical findings, radiographic changes and symptoms | Systemic management, including the use of pain medication and antibiotics | N/A |
| Stage 1 | Exposed and necrotic bone, or fistulae that probes to bone, in patients who are asymptomatic and have no evidence of infection | Antibacterial mouth rinse, Clinical follow-up on a quarterly basis, Patient education and review of indications for continued bisphosphonate therapy |
|
| Stage 2 | Exposed and necrotic bone, or fistulae that probes to bone, associated with infection as evidenced by pain and erythema in the region of the exposed bone with or without purulent drainage | Symptomatic treatment with oral antibiotics, Oral antibacterial mouth rinse, Pain control, Debridement to relieve soft tissue irritation and infection control |
|
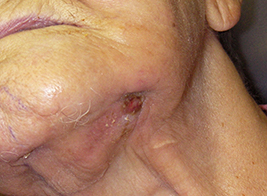
| Stage 3 | Exposed and necrotic bone or a fistula that probes to bone in patients with pain, infection, and one or more of the following: exposed and necrotic bone extending beyond the region of alveolar bone,(i.e., inferior border and ramus in the mandible, maxillary sinus and zygoma in the maxilla) resulting in pathologic fracture, extra-oral fistula, oral antral/oral nasal communication, or osteolysis extending to the inferior border of the mandible of sinus floor | Antibacterial mouth rinse, Antibiotic therapy and pain control, Surgical debridement/resection for longer term palliation of infection and pain |
|